

Five years ago, I traveled to Japan as part of the U.S. Government’s response to the Fukushima Daiichi nuclear accident. With March marking the five year anniversary of Fukushima, this article attempts to highlight some incident management lessons learned and considerations for nuclear and radiological incident management.
This month marks the five year anniversary of the Great East Japan Earthquake. Also known as the 2011 Tohoku earthquake, the 9.0 magnitude undersea quake 43 miles (70 kilometers) off the coast of Japan triggered a powerful tsunami that reached heights of 133 feet (40.5 meters). The devastation was widespread and the human toll was staggering: 15,893 confirmed fatalities, 6,152 injuries, and 2,572 missing, according to the National Police Agency of Japan. Complicating the humanitarian response was the three nuclear meltdowns and release of radioactive materials from the Fukushima Daiichi Nuclear Power Plant. Disasters are never as simple and one-dimensional as we plan for them to be and this turned into an unprecedented and unimaginable trifecta: earthquake followed by tsunami followed by a nuclear disaster. This incident presents some outstanding incident management learning points which I will attempt to highlight in this article.
Fukushima Daiichi Background
Most everyone is familiar with the Fukushima Daiichi nuclear accident, but I will take a moment to set the stage for the incident. This is not intended to be a full technical recap, but simply some facts to ground the discussion.
There is a common misperception that it was the 9.0 earthquake that caused the equipment failures and subsequent nuclear meltdowns at Fukushima. For the most part, the nuclear power plant survived the earthquake and functioned as designed. Following the earthquake, the reactors went into an immediate and automatic shutdown. In the course of this shutdown, as designed, the plant stopped generating electricity and the on-site emergency diesel generators began providing power to circulate coolant water to prevent the nuclear fuel rods from melting down. The system performed as intended for such an anticipated incident. Everything was fine…for the next 40 minutes.
A mere 41 minutes after the earthquake, the first tsunami wave hit, followed by a second 8 minutes later. As a 42.5 foot (13 meter) wave crashed over the seawall protecting the Fukushima Daiichi Nuclear Power Plant from the Pacific Ocean, the real problems began. These waves flooded the emergency diesel generators causing them to fail. At this point, the power supply defaulted to an electrical battery operated emergency pump system and when those batteries ran out on March 12, the real nuclear disaster began.
Over the next few days as plant workers and emergency responders attempted to restore the cooling process, the reactors began to overheat and multiple hydrogen-air chemical explosions occurred, resulting in several releases of radioactive material into the atmosphere. Over the next few weeks there were numerous releases of radioactive material from the reactors, including deliberate venting to reduce gas pressure, deliberate discharge of coolant water into the sea, and uncontrolled releases. When all was said and done, this was the second largest nuclear accident in history, following only Chernobyl, to which the Japanese did their best to respond while also dealing with the widespread devastation from the earthquake and tsunami.
Incident Management Lessons Learned
There has been a considerable amount of research and analysis on the technical aspects of the Fukushima Daiichi nuclear accident, including the nuclear reactor engineering and safety, as well as health and environmental effects from the radiological release. Less attention has been given to the incident management aspects of the nuclear accident and how those can be applied to future nuclear and radiological incidents. Specifically, this article will focus on the following areas:
- Public Fear of Radiation
- Defining the Incident Area
- Dividing the Incident into Manageable Pieces
- “One Plume, One Response”
Fear of Radiation
Radiation is a relatively misunderstood hazard and the risks associated with radiation and radiation exposure are often misconstrued. To start with, not all radiation is bad and it is actually something we are exposed to in small quantities every day. But radiation is an invisible hazard. Undetectable to the human senses, specialized equipment is needed to detect the presence of radiation. The mere mention of radiation among the general public can cause the hair on the back of their neck to stand up, not because it is necessarily dangerous, but because it is unknown, and therefore scary.
The general misunderstanding of radiation and the risk it poses, along with that fear, in itself creates incredible incident management challenges. An all-hazards incident of Type 3 complexity can have the complexity ratcheted up a level or two by introducing a radiological factor to the incident. And this doesn’t necessarily need to be a real radiation threat, just a perceived one; a perceived radiation threat can complicate your incident management efforts. Perception is reality and must be managed as such.
As an example of this unfounded fear, we need to look no further than the United States during the Fukushima incident. All over the U.S., the general public was panicky about the risk posed by the radiological release in Japan. Was the radioactive plume going to travel to the U.S.? (Only detectable in microscopic quantities of absolutely no health or environmental concern.) Was radiologically contaminated debris going to wash up on our shores? (Debris was likely to wash up, but contaminated debris was less likely.) Can we still eat sushi? (Of course!) Should we take Potassium Iodide tablets? (Absolutely not!!)
This fear was especially prominent in West Coast states. In April 2012 I had the opportunity to attend the National Radiological Emergency Preparedness (NREP) Conference where I heard an informative presentation titled “The West Coast Response to Fukushima”. After spending several weeks in Japan as part of the U.S. Government’s response to Fukushima in the spring of 2011, I wondered, “What was the West Coast response? I thought this whole thing was in Japan.”
What I was about to learn was that despite a nearly 5,000 mile distance between Fukushima Daiichi and the West Coast of the continental U.S., the effects of the incident had considerable impact on the U.S. mainland, and the West Coast states in particular. By effects, I do not mean significantly elevated radiation readings that cause health or environmental concern (because that didn’t happen), but challenges associated with managing public perception and communicating technical information about the hazards (or non-hazards) to the public.
The presentation given by public health professionals from Washington State and Orange County, CA, told a story of emergency managers and public health professionals who were faced with a rather complex challenge of communicating with the public, explaining the technical details of Fukushima and radiation exposure in a relatable and non-technical manner, while allaying the fear, managing public perception, and maintaining public confidence. They were peppered with questions like “Is it safe for my grandchildren to play outside?” All of this was in response to an incident occurring in another country over 5,000 miles away and a potential hazard that should not have risen to any level of concern on our shores.
In response to these questions and the associated public hysteria, Emergency Operations Centers across the West Coast were in some state of operational activation for several months. The response was not an “operational” response in the sense that they were deploying and coordinating field resources, rather, the response was a public information campaign, focused on educating the public and communicating technical information in a non-technical manner to the layman.
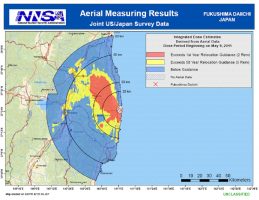
![]() Defining the Incident Area
Defining the Incident Area
So when you are faced with a scenario such as the one described in the previous section, what is the “incident area” and how do you define your “area of operations”? I want to draw your attention to a quote from the National Incident Management System (NIMS) document:
“Acts of biological, chemical, radiological, and nuclear (commonly referred to as CBRN) terrorism may present unique challenges for the traditional ICS structure. Incidents that are not site specific, are geographically dispersed, or evolve over longer periods of time will require extraordinary coordination among all participants, including Federal, State, tribal, and local governments, as well as NGOs and the private sector.”
While Fukushima was not an act of terrorism, this statement holds true; natural disasters and technological failures can present the same CBRN incident management challenges as terrorism incidents, especially in a nuclear or radiological incident.
I want to focus on “…incidents that are not site specific, are geographically dispersed…” One might say that Fukushima was site specific because you can point to a spot on a map where the nuclear power plant was located, but the real radiation hazard, and perceived radiation hazard, were anything but site specific. While you can look at the DOE/NNSA contamination maps from Japan to see more “tangible” threats, you need to look no further than the “West Coast response to Fukushima” to see the impact of perceived threats to areas outside of the designated area of operations. Even with no measurable radiation reading indicating anything close to a threat to public health or the environment, the West Coast was still dealing with an “incident”, albeit non-traditional.
I draw your attention to this because it helps us understand the challenges with defining the “site” or “area of responsibility”. The invisible hazard coupled with the common lack of understanding of the radiation hazard, makes it hard to define, and thus limit, the affected area. In fact, it could be argued that public misunderstanding expands the incident area. Furthermore, operational resources may be allocated in response to public or political demands to “validate zeroes” and prove there is no radiological hazard in areas far from the real hazard. From a radiological incident management perspective, both operational and public messaging, the area of responsibility can extend a long, long way, creating geographic and span-of-control challenges. In summary, the “incident area” may be larger than you think.
Dividing the Incident into Manageable Pieces
We all know about span-of-control and we may even remember from our ICS-400 class the concept of dividing a single incident into two or more incidents when it gets too large to manage under one Incident Command organization. Given the fact that there was a “West Coast response to Fukushima” 5,000 miles away from the incident origin, we can confidently assume there may be a need to divide a large scale nuclear or radiological incident among multiple Incident Command organizations, each with separate and distinct geographic areas of responsibilities.
When I talk about dividing an incident in response to a nuclear or radiological incident, I focus on four basic steps:
1) Incident Size Up
2) Prioritization of Geographic Areas
3) Breaking the Incident into Manageable Pieces
4) Allocating Resources to Each Area
Incident size-up in this case is not dissimilar to routine incident size-up, it just needs to be viewed from a larger perspective. It is not solely focused on the incident origin location, but also considers:
- Initial models and predictions
- Downwind effects
- Populations impacted and potentially impacted
- Jurisdictional boundaries
- Resource availability
- Potential areas of operational concern vs. potential areas of public perception concern
Once this size-up is conducted, incident managers can begin to identify priority areas. This may include prioritizing geographic areas by the radiological hazard and risk. Are certain areas susceptible to greater public health risk than others? Is there a short-term exposure risk vs. a long-term exposure risk? What are the environmental or agricultural concerns (ingestion pathway)? Are there critical infrastructure or political considerations? Are there public perception or public confidence issues that need to be considered?
After size-up and identification of geographic priorities, decisions about breaking the incident into manageable pieces can be discussed. The list below is adapted from a checklist in the Beyond Initial Response Incident Command System textbook that identifies considerations for dividing the Operations Section into geographic Divisions. Considerations when dividing a large incident into two or more incidents should include:
- Size of affected area
- Priorities
- Complexity of the incident and the hazard
- Capabilities and experience of available resources
- Amount of work to be accomplished
- Functions to be accomplished
- Span-of-control issues
- Operating environment
- Topography
- Natural boundaries and barriers
- Political and jurisdictional issues
- Logistics requirements
Lastly, once the incident is divided into manageable pieces, resources should be allocated to each incident area. This should include not only technical response resources (critical radiological response resources), but management and overhead resources (Incident Management Teams). Incident managers should also consider the use of Area Command at this time, with multiple Incident Command Posts managing smaller geographic areas of responsibility reporting to an Area Command Post with responsibility for a larger geographic area.
“One Plume, One Response”
For seasoned incident management professionals, dividing a large, complex incident into manageable pieces is not a foreign concept, but dividing a radiological incident is not as simple as dividing a large wildfire or earthquake or hurricane response. In radiological response, there is a technical connectivity from one geographic end of the incident area to the other unlike in other all-hazards incidents. In other all-hazards incidents responders can typically work at one end of the impact zone with little coordination and communication with responders on the other end. But in radiological response, the data and samples collected, regardless of where, help inform the overall common operating picture that impacts health, safety, and environmental decisions. This is why radiological responders often use the term, “One Plume, One Response”. It implies that regardless of jurisdictional boundaries, or any other reason to divide the incident, they manage the response from a big picture perspective.
So while the field level response may be broken into manageable pieces, each with separate and distinct areas of responsibility, the technical response from a data management and assessment standpoint is still looking at the big picture. This creates challenges with maintaining a Common Operating Picture across a large geographic area. Included in this are challenges associated with information and data management, public messaging, consistent decision-making, and critical resource allocation. This is another reason why Area Command should be considered when managing large scale nuclear or radiological incidents.
Summary
The Fukushima Daiichi nuclear accident, as well as the earthquake and tsunami, were horrific disasters. While we hope they aren’t repeated, we know that even if they aren’t there will one day be another incident of equal or greater complexity. Keys to successful large scale nuclear or radiological incident management must include:
- Effective public communications and messaging
- Recognition of the size and scope of the incident, to include not just the radiological deposition footprint, but the scope of the public information response
- Making the incident manageable by using the flexibility of the Incident Command System (ICS)
- Maintaining an incident wide Common Operating Picture of the radiological hazard to inform consistent decision-making
Not only does this type of incident create challenges for the traditional ICS structure, but it will challenge the entire NIMS Command and Management framework of ICS, Multiagency Coordination, and Public/Joint Information. To be successful, it will require a highly coordinated, multiagency and multijurisdictional response to successfully manage it.
About the Author
Billy Haley is the Director of Operations for EMSI (https://www.emsics.com/#!billy-haley/cwm1). Prior to joining EMSI, he worked as a contractor with the U.S. Department of Energy/National Nuclear Security Administration. In March 2011, he responded to Japan with DOE/NNSA as part of the U.S. Government response to Japan. For his contributions, Billy earned the DOE Secretarial Honor Award and the U.S. Agency for International Development (USAID) Meritorious Group Award. Recognized as an expert in nuclear and radiological incident management, Billy has presented at the National Radiological Emergency Preparedness (NREP) conference, Health Physics Society, and several government seminars of nuclear and radiological response.